Brief description
A Coordinate My Care (CMC) user views a patient’s urgent care plan and, along with the existing care plan data, can see current medications pulled in real time from the GP system relevant for that patient.
For the purpose of the use case, we will assume an urgent care user of CMC, such as a paramedic working for the London Ambulance Service (LAS). However, CMC is used in emergency, primary, and secondary services, and clinicians from all these areas also access CMC urgent care plans for patients in Greater London.
The following list comprises the types of urgent care users who will utilise the information:
- Doctor in A&E department
- Nurse in A&E department
- Clinical adviser in 111 service
- Out of hours (OOH) GP
- Paramedic from ambulance service
Smartcard access is not required to access CMC. Many users log in with a CMC user name and password. A smartcard is one of the options they have available to them. For EMIS practices, we have implemented single sign-on, which allows us to link the EMIS user account to the CMC account and provides a way for them to access the application from within EMIS Web.
Use case justification
This use case focuses on patient safety – where a wide range of clinicians who currently do not have access to patient current medication could have this information available to them.
In Greater London, the CMC urgent care plan is accessed by urgent and non-urgent care providers who can view key information, assisting decision-making in urgent and non-urgent care scenarios. Anticipatory medication is included in the care plans, but due to the dynamic nature of current medication, ‘current medication’ is not included in care plan data. The GP connect service would allow CMC to pull this data in real time, ensuring the most up-to-date view of medication on the GP system is reflected on the CMC plan safely. CMC currently requires the user to input urgent care medications and does not pull them from any other data source.
This information could be used in urgent, acute, primary and community settings, as CMC is used by clinicians in all these areas across Greater London. CMC is used by approximately 30 urgent care providers including LAS and North West London (NWL) 111.
CMC is a web-based application that supports the development of an urgent care plan for a patient. Many users across different care settings collaborate on a single version of the truth for a patient. This application is accessed over an N3 network. The application is available over non-N3 using two-factor authentication which is made available to organisations on a case by case basis. Many hospices do not have N3 access, so they would be required to comply with our mini information governance (IG) toolkit before access is provided using this method.
Intersystems is our technology partner and we have procured a solution which encompasses many of its technologies. We are currently working on a rollout to extend access to users by enabling it to be launched from their own native system. This is currently in place with EMIS Web and in a test environment for Homerton University Hospital NHS Trust.
1,000+ GP practices (covering TPP, EMIS, Microtest and INPS)
Currently CMC can be launched from within EMIS Web in patient context. The system does not update EMIS, but it allows the user to access CMC from within a patient record using the Portal SDK functionality.
The number of EMIS practices in London is in the region of 960. Over 500 practices have completed the configuration to access CMC from EMIS Web. We are looking to promote this to extend usage beyond GP practices into community.
35 acute hospitals
Currently CMC is accessed via the URL shared above. There are plans to roll out a similar in-context launch from acute systems and this has so far been achieved in a test environment with the Homerton who use Cerner Millennium.
20 hospices
Please see the responses above.
CMC is not reliant on SNOMED codes for this use case. We may be interested in doing the mapping to future-proof the CMC solution.
Currently in Greater London approximately 100 CMC plans are viewed per day. At this point, we don’t have figures on time-of-day, but many will be viewed in out-of-hours scenarios. For planning purposes, we should assume that every time an urgent care plan is viewed, the medications section will be viewed (which is likely).
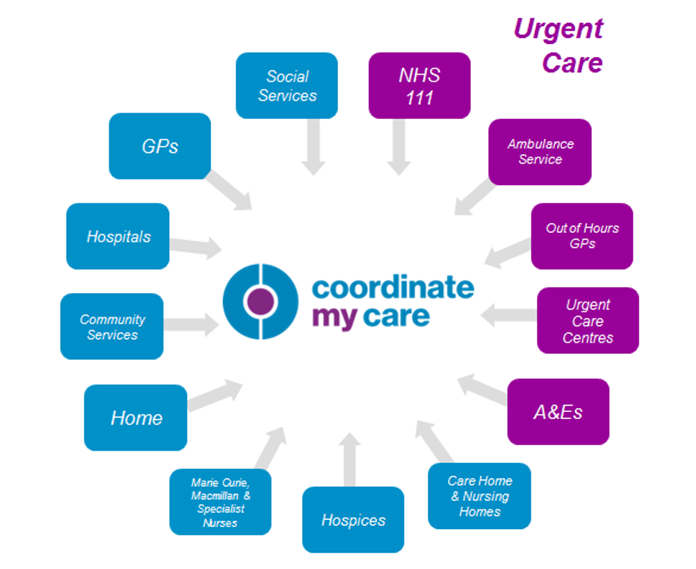
Fig. 1 – Types of organisations using CMC, urgent and non-urgent
It is projected that the annual cost of admissions related to adverse drug reactions to the NHS is £466 million, and over 70% of these admissions are thought to be avoidable1.
CMC offers multidisciplinary monitoring and updating of medications in real time. This has patient safety and cost applicability to medications such as:
- Anti-coagulations services
- Drug abuse programmes
- Medications documented on CMC urgent care plan for patients at the end of their lives, enabling community services to administer medications required to keep patients comfortable in their own homes, thus avoiding unnecessary hospital admissions.
An interoperability solution with GP systems for current medication will also mitigate any risks associated with manual entry of current medication to non-GP systems, including transcription errors and information becoming out of date. This would also save time for any clinicians who currently manually transcribe this to other systems but who could access this information via CMC.
Primary actors
- CMC urgent care user (London Ambulance Service paramedic, OOH GP, 111 and A&E staff)
- CMC non urgent care user (acute hospital clinician, community nurse, allied health professional, social worker)
- GPs
Triggers
- Urgent care user accesses CMC urgent care plan and navigates to medication page of that patient’s plan.
Preconditions
- Patient is registered to a GP in one of the 32 Greater London CCGs covered by CMC.
- Current medications have been populated in GP system and this is available to GP connect.
- Care plan has been created in CMC for relevant patient.
- Urgent care actor is a registered CMC user and user’s organisation has signed internet service agreement (ISA) and acceptable use policies.
Postconditions
- On success
- When accessing the medications page on the CMC care plan, all current medications available in the relevant GP system are presented to the user instantly, in real time.
- Guaranteed
-
The request to pull data and the outcome (successful/unsuccessful) with other metadata is logged and auditable.
-
It is clear to the user where the call has been completed and there are no current medications captured (‘none’ or similar message is presented).
-
It is clear to the user where the GP connect service is not contactable (‘GP system not available’ or similar message is presented).
-
Basic flow with alternative and exception flows
| Step | Description |
|---|---|
| Step 1 | CMC user logs into CMC from N3 network (or on non-N3 via authentication partner authen2cate). |
| Step 2 | CMC urgent care user accesses a patient’s CMC plan. |
| Step 3 | CMC confirms the patient’s GP practice using Personal Demographics Service (PDS)/Spine Directory Service (SDS) lookup. |
| Step 4 | Urgent care user clicks on the medications tab within CMC system. |
| Step 5 | CMC requests the patient’s ‘Current Medication List’ from their registered GP practice. Current medication – medication prescribed to the patient (as either a single prescription or an instance of a repeat prescription) within the last three months. |
| Step 6 | Spine Security Proxy (SSP) checks organisation to organisation sharing agreement exists between requesting organisation (doctors) and the patient’s registered GP practice, and that the interaction (e.g. Get Medications) is part of the sharing agreement. |
| Step 7 | GP practice clinical system checks patient permissions and consent to share. |
| Step 8 | CMC receives the ‘Current Medication List’ and presents the results to the clinician. The following information is returned with the following information:
Format to be confirmed but could be presented so as similar to GP system medication page layout. |
| Step 9 | CMC will import the medication information into a temporary storage. This will include mapping the data received into the CMC own data structures/coding for medications. |
| Step 10 | CMC user is then able to view current medications and act accordingly. |
| Exceptions | |
| Step 2a | GP practice is not found on SDS. |
| Step 3a | No medications returned. |
| Step 4a | Patient not returned. |
| Step 5a | Patient consent not given. |
| Step 6a | GP Connect connectivity down. |
| Step 7a | Current medication is updated by GP and CMC user re-checks |